
Cystic Duct Closure Devices Remain Competent Beyond ERCP-Generated Pressures
Caleb Hammond
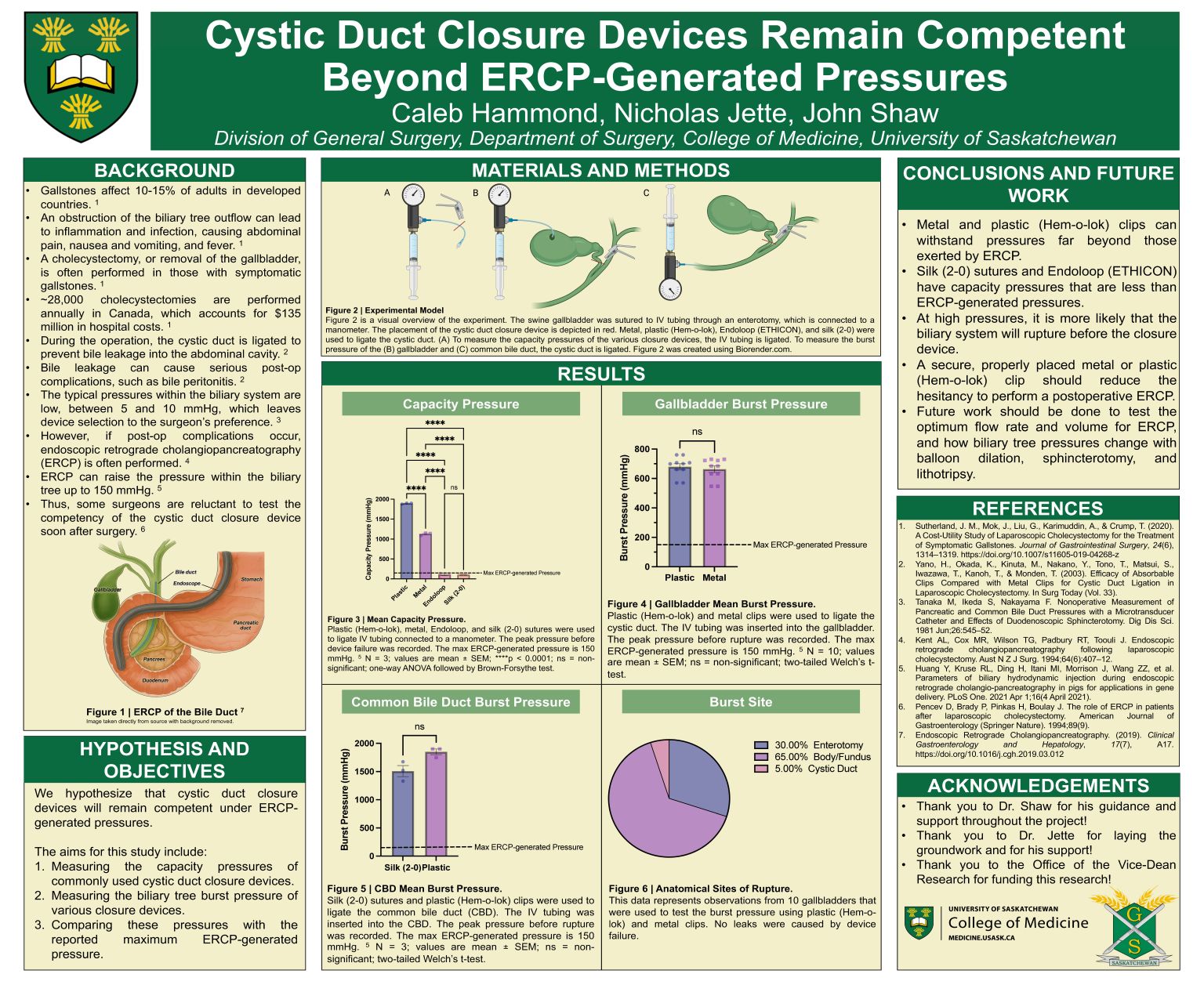
Gallstones are a prevalent and costly disease in Canada, often requiring gallbladder removal
(cholecystectomy). During the operation, the cystic duct is ligated to prevent bile leakage into the
abdomen. Since the intraluminal biliary pressures are relatively low, the closure device used is left
to the surgeon’s preference. However, post-operative complications, such as recurrent stones, can
be treated with endoscopic retrograde cholangiopancreatography (ERCP), which can raise the
pressures to 150 mmHg, according to a recent study. For this reason, surgeons are hesitant to
perform ERCP soon after surgery. This study tested the competency of various commonly used
cystic duct closure devices and compared them against the reported maximum ERCP-generated
pressure. Using IV tubing, we examined the capacity pressures of various closure devices. We also
used swine gallbladders and bile ducts to determine the burst pressure of the biliary system when
the cystic duct is ligated. Our results suggest that metal and plastic (Hem-o-lok) clips have capacity
pressures beyond the maximum ERCP-generated pressures. Moreover, high pressures are more
likely to rupture the biliary system than cause device failure. Overall, our data indicates that a
secure and properly placed device should mitigate the hesitancy to perform a post-operative ERCP.