
A Prospective Analysis of Patients with Nonflaccid Facial Paralysis Undergoing Chemodenervation versus Selective Neurectomy
Ayeh Aldulaymi
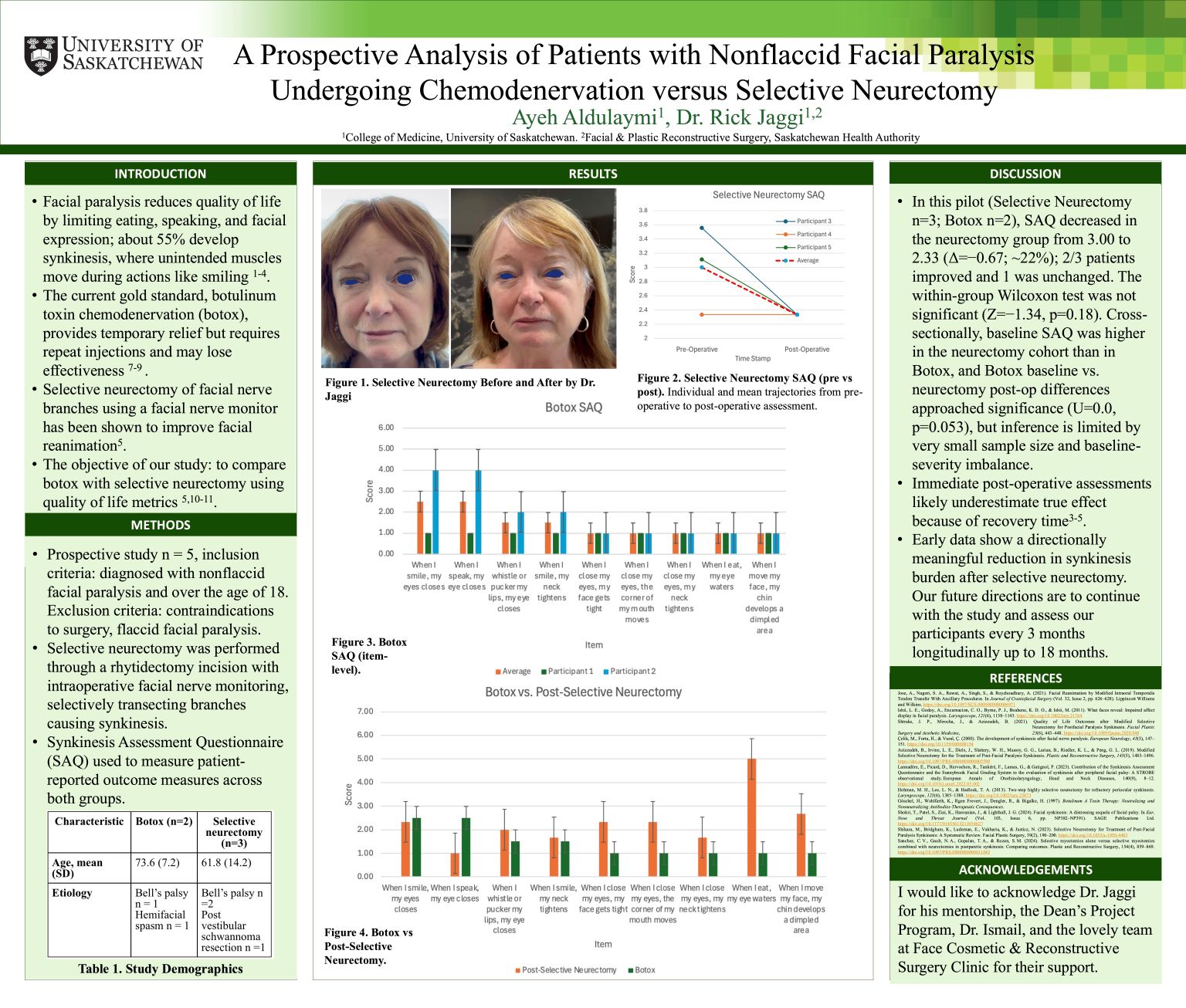
Background: Nonflaccid facial paralysis (NFFP) with synkinesis impairs function and quality of life. Botox is effective but temporary, selective neurectomy targets durable reduction of co-contraction. Prospective patient-reported comparisons are not reported.
Methods: We conducted a single-centre prospective pilot. Adults with NFFP received selective neurectomy (n=3) or botox (n=2). The Synkinesis Assessment Questionnaire (SAQ; 9 items, higher=worse) was collected at baseline, selective neurectomy patients were reassessed immediately post-op. Primary tests were Wilcoxon signed-rank (within neurectomy) and Mann-Whitney U (between groups).
Results: In selective neurectomy, mean SAQ fell from 3.00 to 2.33 (Δ=−0.67; ~22%); 2/3 improved and 1/3 was unchanged. The change was not significant (Z=−1.34, p=0.18). Baseline SAQ was higher in selective neurectomy than botox (U=0.0, p=0.08). Comparing botox baseline with selective neurectomy post-op approached significance (U=0.0, p=0.053). Item-level trends showed reduced peri-orbital co-contraction, with persistent gustatory lacrimation in some.
Conclusions: Immediate post-op findings show directionally favourable change after selective neurectomy but no statistical significance in this underpowered pilot. Because recovery in NFFP is time-dependent (edema resolution, reinnervation, rehabilitation), immediate assessment likely underestimates benefit. Ongoing 3-monthly follow-up to 18 months will define trajectories, refine effect sizes, and clarify the roles of durable selective neurectomy versus repeat botox in patient-centred care.