
A1.4: Dexamethasone-supplemented TAP blocks may reduce opioid requirements after colorectal surgery: a retrospective study
Nawaf Abu-Omar, Zarrukh Baig, Nathan Ginther, Dilip Gill
Background: The transversus abdominis plane (TAP) block is a peripheral nerve block that reduces postoperative opioid requirements. The use of dexamethasone in conjunction with peripheral nerve blocks has been proven to be an effective adjunct, however, its use remains off-label. The objective of this study was to assess pain control in the first 48 post-operative hours after minimally invasive colorectal surgery in patients who received laparoscopically placed TAP blocks with and without perineural dexamethasone.
Methods: Sixty patients undergoing laparoscopic colorectal surgery were included in this study. Patients were allocated into 2 groups. Group 1 (TAP) received bilateral TAP blocks using 0.25% bupivacaine with epinephrine and Group 2 (TAP-D) received bilateral TAP blocks using 0.25% bupivacaine with epinephrine in combination with dexamethasone. Patient demographics, wound class, opioid use in the post anesthetic care unit, at 24h, 48h, use of patient-controlled analgesia (PCA) and length of stay were recorded.
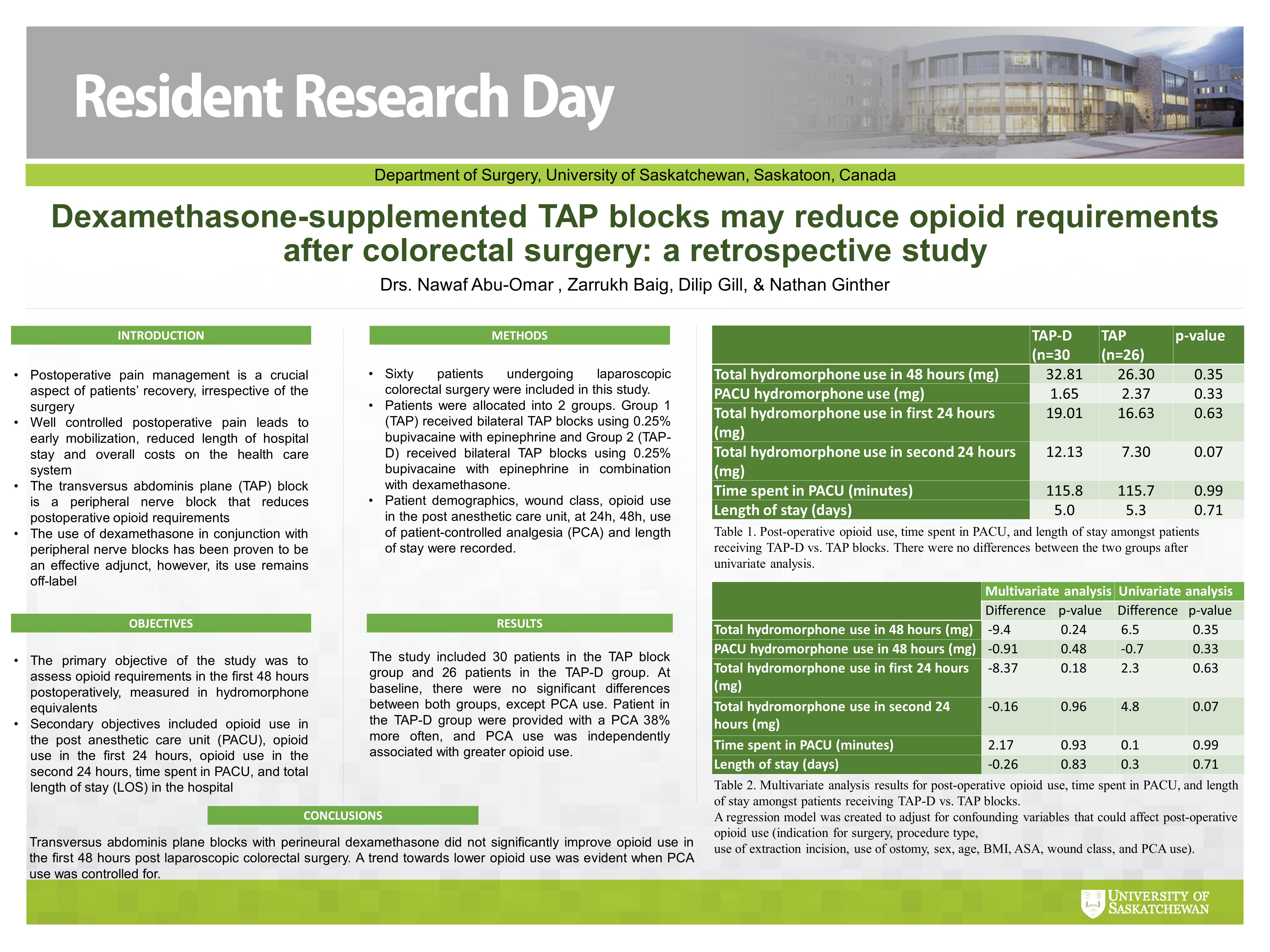
Results: The study included 30 patients in the TAP block group and 26 patients in the TAP-D group. At baseline, there were no significant differences between the characteristics of both groups, including surgical indication and technique, except PCA use. Patients in the TAP-D group were provided with a PCA 38% more often, and PCA use was independently associated with greater opioid use. For outcomes, transversus abdominis plane blocks with perineural dexamethasone did not significantly change opioid requirements in PACU, at 24H or 48H post-op. A multivariate analysis adjusting for 10 confounders, including PCA use, found a trend towards lower opioid use in the first 48 hours with TAP-D (-9.4mg), however, it was not significantly different (P=0.242).
Conclusion: Transversus abdominis plane blocks with perineural dexamethasone did not significantly improve opioid use in the first 48 hours post laparoscopic colorectal surgery. A trend towards lower opioid use was evident when PCA use was controlled for.